Overview
The abomasum, the fourth compartment of the ruminant stomach, is analogous to the monogastric stomach and plays a crucial role in enzymatic digestion. Abomasal disorders are significant in bovine medicine, particularly in high-producing dairy cattle, and are commonly assessed on the NAVLE.

1. Displaced Abomasum (DA)
Displaced Abomasum (DA)
Classic Presentation
- Species/Breed: Dairy cows, especially multiparous individuals
- Timing: Typically occurs within 30 days post-calving
- Signs:
- Partial anorexia
- Gradual weight loss
- Scant stool with inconsistent consistency compared to herdmates
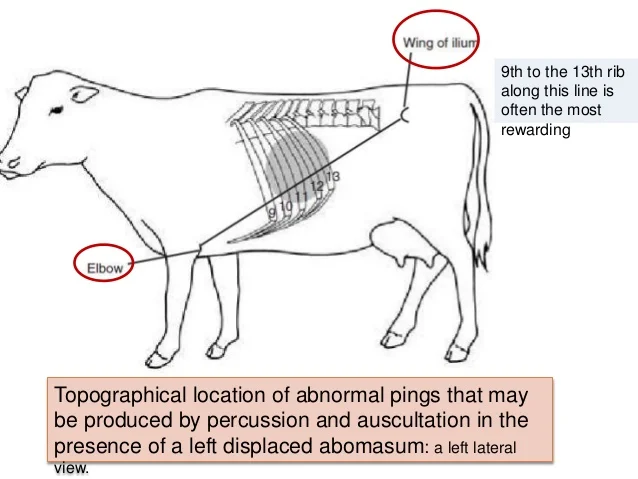
- “Sprung” or “popped” rib cage: Ribs appear pulled outward
- High-pitched tympanic “ping” on auscultation/percussion
Ping Locations
- Left Displaced Abomasum (LDA):
- Ping found along line between left elbow and left tuber coxae
- Right Displaced Abomasum (RDA) or Right-Torsed Abomasum (RTA):
- Ping on right side
- RTA-specific signs:
- Tachycardia
- Papple-shaped abdomen: pear on left, apple on right
- Colic
- Dehydration
Diagnosis
- Ping: Most commonly diagnostic on physical exam
- Rectal Palpation:
- May palpate a convex, muscular structure in the right abdominal quadrant (suggestive of RDA or RTA)
- Metabolic Abnormalities:
- Hypochloremic metabolic alkalosis due to HCl sequestration
- May progress to metabolic acidosis in cases with circulatory collapse
- Liptak Test:
- Insert 4.5-inch spinal needle ventral to the area of the ping
- Aspirate fluid
- Acidic fluid confirms abomasal content
Treatment
Medical Management:
- Non-surgical correction:
- Roll-and-toggle procedure
- Blind stitch technique
- Supportive therapy:
- Calcium supplementation
- Transfaunation (rumen fluid transfer)
- Gastric stimulants
Surgical Options:
- Abomasopexy: Surgical fixation of abomasum
- Omentopexy: Anchoring via the omentum
Key Points / Pearls
- Prognosis:
- Generally excellent for both survival and return to productivity
- Emergency Status:
- LDA: Not an emergency
- RDA/RTA: True emergencies requiring prompt intervention
- Herd-Level Management:
- Investigate and intervene if DA prevalence exceeds 1% in the herd
- Preventive strategies:
- Focus on pre-partum nutrition to support abomasal motility
Left Displaced Abomasum (LDA)
- Pathophysiology: The abomasum moves from its normal position on the right ventral abdomen to the left side, becoming trapped between the rumen and the left abdominal wall.Scribd
- Risk Factors: High-producing dairy cows, particularly within the first month postpartum, are at increased risk. Factors include abomasal hypomotility, concurrent diseases (e.g., ketosis), and dietary changes.Quizlet
- Clinical Signs: Decreased appetite, reduced milk production, and a characteristic “ping” on auscultation over the left abdomen.
- Diagnosis: Based on clinical signs and confirmation via ultrasound or exploratory surgery.
- Treatment: Surgical correction (e.g., right flank omentopexy) or less commonly, rolling and toggling techniques.
Right Displaced Abomasum (RDA) and Abomasal Volvulus
- Pathophysiology: The abomasum displaces to the right side; in volvulus, it twists on its mesenteric axis, leading to vascular compromise.Scribd
- Clinical Signs: Similar to LDA but may progress rapidly to signs of shock in volvulus cases.Scribd+1Scribd+1
- Diagnosis: Clinical examination and imaging.Scribd+2icva.net+2prezi.com+2
- Treatment: Emergency surgical intervention is required for volvulus.

2. Abomasal Ulcers
- Types:
- Type I: Non-perforating, superficial erosions.
- Type II: Ulcers with significant bleeding.
- Type III: Perforating ulcers with localized peritonitis.
- Type IV: Perforating ulcers with diffuse peritonitis.
- Risk Factors: Stress, high-concentrate diets, NSAID use, and concurrent illnesses.
- Clinical Signs: Anorexia, melena, abdominal pain, and signs of sepsis in perforating ulcers.
- Diagnosis: Clinical signs, fecal occult blood tests, and imaging.
- Treatment: Dietary management, antacids, H2 blockers (e.g., ranitidine), and surgical intervention for perforating ulcers.
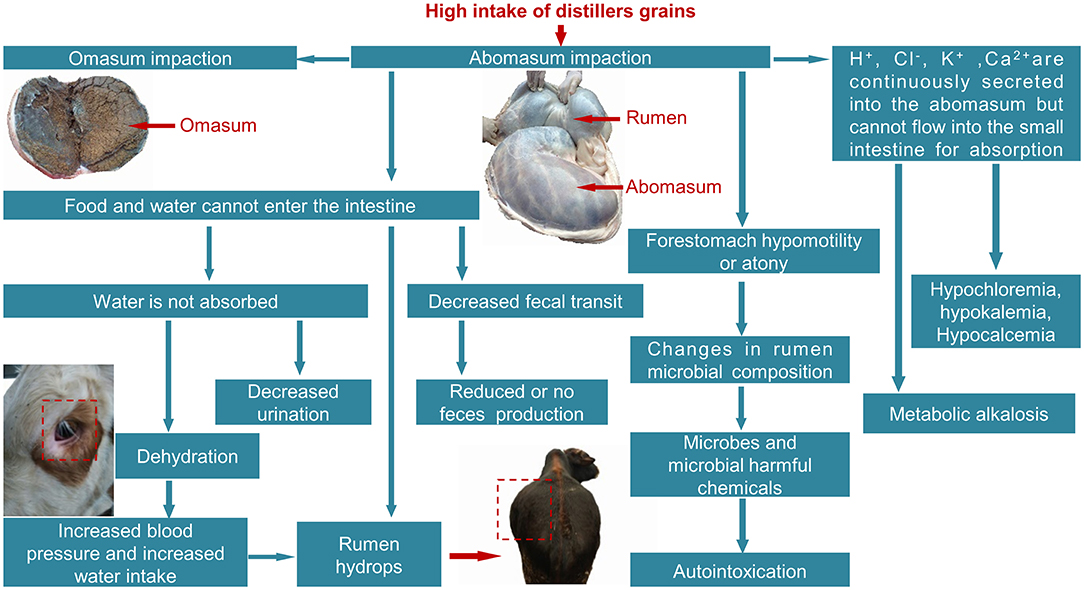
3. Abomasal Impaction
- Etiology: Ingestion of indigestible materials or poor-quality forage leading to obstruction.
- Clinical Signs: Anorexia, decreased fecal output, abdominal distension, and dehydration.
- Diagnosis: Physical examination, imaging, and exploratory surgery.
- Treatment: Oral laxatives (e.g., magnesium sulfate), intravenous fluids, and possibly rumenotomy to remove impacted material.
4. Abomasal Torsion/Volvulus
- Pathophysiology: The abomasum twists on its axis, leading to vascular compromise, necrosis, and rapid deterioration.Scribd
- Clinical Signs: Severe abdominal pain, rapid onset of shock, and distension of the right abdomen.
- Diagnosis: Clinical signs and imaging.
- Treatment: Immediate surgical correction is essential.www.slideshare.net+7Brainscape+7ResearchGate+7
NAVLE-Style Multiple-Choice Questions
Question 1: Diagnosis of Displaced Abomasum
Clinical Scenario:
A 4-year-old Holstein cow, 10 days postpartum, presents with decreased appetite and milk production. On auscultation, a “ping” is heard on the left side between the 9th and 13th ribs.
Question:
What is the most likely diagnosis?
A. Left displaced abomasum
B. Right displaced abomasum
C. Cecal dilation
D. Rumen tympany
E. Abomasal impactionSemantic Scholar+11vettimes.co.uk+11vettimes.co.uk+11Merck Veterinary Manualicva.net
Correct Answer: A. Left displaced abomasum
Explanation:
The “ping” on the left side in a postpartum dairy cow is characteristic of a left displaced abomasum.
Question 2: Management of Abomasal Ulcers
Clinical Scenario:
A beef cow presents with melena and signs of anemia. Fecal occult blood test is positive.
Question:
What is the most appropriate initial management?
A. Immediate surgical intervention
B. Administration of NSAIDs
C. Dietary management and H2 blockers
D. High-concentrate feeding
E. No treatment necessary
Correct Answer: C. Dietary management and H2 blockers
Explanation:
Non-perforating abomasal ulcers can often be managed with dietary adjustments and medications like ranitidine to reduce acid secretion.
Question 3: Treatment of Abomasal Impaction
Clinical Scenario:
A cow exhibits decreased fecal output and abdominal distension after consuming poor-quality forage.
Question:
Which treatment is most appropriate?
A. High-concentrate feeding
B. Administration of magnesium sulfate and fluids
C. Surgical correction via omentopexy
D. Use of NSAIDs
E. Immediate slaughter
Correct Answer: B. Administration of magnesium sulfate and fluids
Explanation:
Abomasal impaction due to indigestible forage can often be relieved with oral laxatives like magnesium sulfate and supportive fluid therapy.