Pericarditis—the inflammation of the pericardial sac surrounding the heart—is an important condition in bovine medicine and a high-yield topic for the NAVLE. This guide distills the clinical reasoning, diagnostics, and treatment strategies you need to master to succeed on exam day.
Etiology
The most prevalent form in cattle is traumatic pericarditis, resulting from the ingestion of sharp foreign objects (e.g., nails, wires) that penetrate the reticulum, diaphragm, and subsequently the pericardial sac. This penetration introduces pathogens and foreign material into the pericardial space, leading to inflammation and effusion.
Other causes include:
- Infectious agents: Bacterial infections such as Trueperella pyogenes and Pasteurella multocida.
- Neoplastic conditions: Tumors affecting the pericardium.
- Idiopathic origins: Cases where no definitive cause is identified.
Etiology: Understanding the Underlying Cause
In cattle, traumatic pericarditis is the most common form. It usually results from ingestion of sharp foreign bodies (such as wires or nails) that perforate the reticulum and extend into the pericardial sac, causing inflammation and fluid accumulation.
Other causes include:
- Bacterial infections (e.g., Trueperella pyogenes, Pasteurella multocida)
- Viral infections (less common)
- Neoplastic involvement
- Idiopathic pericarditis
Clinical Signs: What to Look For
NAVLE clinical vignettes often test your ability to recognize key physical signs. Know the following:
Cardiovascular and systemic findings:
- Decreased feed intake and milk production
- Jugular vein distension
- Brisket or ventral subcutaneous edema
- Muffled heart sounds or pericardial friction rubs
- Tachycardia
- Signs of right-sided heart failure
- Classic “pear-shaped” abdominal appearance (from ascites)
Infectious cases may also show:
- Fever
- Tachypnea
- Depression
Diagnostic Approach
ECG-and-Echocardiogram-showing-pericarditis-pericardial-effusion-related-to-radiation
1. Clinical Exam
- Evaluate for brisket edema, heart sounds, jugular distension
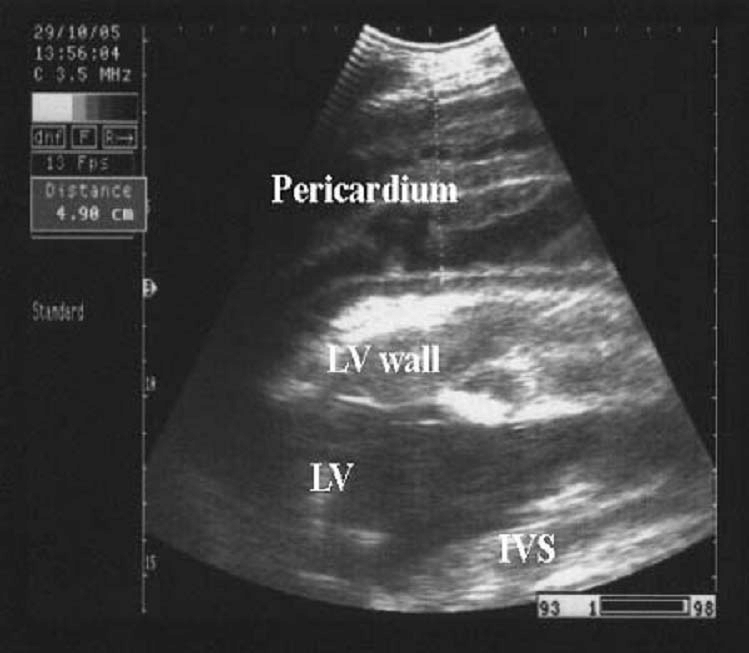
2. Ultrasonography
- Most reliable diagnostic tool
- Findings: hypoechoic pericardial fluid, echogenic fibrin strands, thickened pericardium, or metallic foreign body
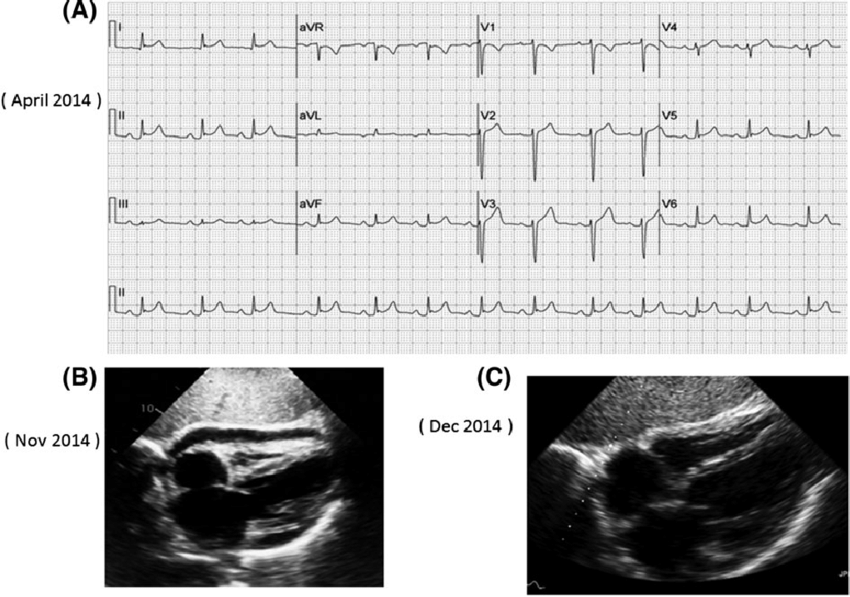
3. ECG
- May reveal low-voltage QRS complexes and ST-segment elevation due to fluid insulation
4. Blood Tests
- Inflammatory leukogram
- Hyperfibrinogenemia
- Elevated globulins
5. Radiography
- May reveal foreign metallic objects in or near the reticulum
Treatment Strategies
NAVLE examiners often want to know what to do first. Here’s the clinical management ladder:
1. Broad-spectrum antibiotics
- Penicillin or oxytetracycline
- Necessary for bacterial or septic cases
2. NSAIDs
- Flunixin meglumine is preferred for anti-inflammatory and analgesic effects
3. Pericardiocentesis
- Emergency procedure to relieve cardiac tamponade caused by fluid accumulation
- Temporary relief of signs
4. Surgery
- Rumenotomy to remove the foreign body from the reticulum
- Pericardiectomy may be required in valuable cases to manage chronic or constrictive pericarditis
5. Supportive therapy
- Fluid and nutritional support
- Environmental management
Differential Diagnoses
NAVLE may ask you to distinguish pericarditis from other causes of edema or cardiac dysfunction. Know how to differentiate:
| Condition | Key Differentiating Features |
|---|---|
| Endocarditis | Valvular murmurs, embolic disease |
| Right-sided heart failure | Edema without muffled heart sounds |
| Traumatic reticuloperitonitis | Withers pinch pain, no pericardial rub |
| Pleuropneumonia | Harsh lung sounds, pyrexia, pleural effusion |
Classic NAVLE Clues
Recognize these as high-yield signs for exam questions:
- Brisket edema in a cow with muffled heart sounds
- Ultrasonographic findings of pericardial fluid with echogenic strands
- History of wire ingestion
- ECG with low voltage and ST elevation
These findings are commonly used in case-based multiple-choice questions.
Summary of Key Points
- Pericarditis in cattle is most commonly traumatic in origin, associated with penetrating metallic foreign bodies from the reticulum.
- Clinical signs include muffled heart sounds, jugular distension, brisket edema, and reduced production.
- Ultrasound is the diagnostic tool of choice; ECG and radiography are supportive.
- Treatment includes antibiotics, NSAIDs, and pericardiocentesis. Surgical removal of the causative object is sometimes necessary.
- Know your differentials and be prepared to identify distinguishing clinical and diagnostic features.
NAVLE-Style Multiple-Choice Questions
Question 1: Diagnosis
Clinical Scenario:
A 5-year-old Holstein cow presents with decreased appetite, reduced milk production, and signs of discomfort. Physical examination reveals jugular vein distension, brisket edema, and muffled heart sounds. An ultrasound of the thoracic region is performed.
Ultrasound Findings:
- Thickened pericardium
- Hypoechoic pericardial effusion
- Fibrin strands within the pericardial sac
Question:
What is the most likely diagnosis?
A. Endocarditis
B. Traumatic pericarditis
C. Myocarditis
D. Pleuropneumonia
E. Congestive heart failure
Correct Answer: B. Traumatic pericarditis
Explanation:
The clinical signs of jugular vein distension, brisket edema, and muffled heart sounds, along with ultrasonographic findings of pericardial effusion and fibrin strands, are characteristic of traumatic pericarditis. This condition often results from the penetration of sharp foreign objects, such as wires, from the reticulum into the pericardial sac, leading to inflammation and fluid accumulation.
Question 2: Treatment
Clinical Scenario:
A 6-year-old beef cow is diagnosed with traumatic pericarditis. She exhibits signs of cardiac tamponade, including tachycardia and muffled heart sounds. Immediate intervention is required to relieve pressure on the heart.
Question:
Which of the following is the most appropriate initial treatment?
A. Administration of diuretics
B. Pericardiocentesis
C. Oral NSAIDs
D. Intravenous fluids
E. Thoracocentesis
Correct Answer: B. Pericardiocentesis
Explanation:
Pericardiocentesis is the procedure of choice to relieve pressure from accumulated fluid in the pericardial sac, especially in cases of cardiac tamponade. This intervention allows the heart to function more effectively by removing the excess fluid. While NSAIDs and antibiotics are important in managing inflammation and infection, they do not provide immediate relief from tamponade.
Question 3: Differentials
Clinical Scenario:
A 4-year-old dairy cow presents with signs of heart failure, including jugular vein distension and brisket edema. An ECG is performed, revealing low voltage QRS complexes and ST segment elevation.
Question:
Which of the following conditions is most consistent with these ECG findings?
A. Myocardial infarction
B. Pericarditis
C. Ventricular tachycardia
D. Atrial fibrillation
E. Pulmonary embolism
Correct Answer: B. Pericarditis
Explanation:
Low voltage QRS complexes and ST segment elevation on an ECG are indicative of pericarditis. The low voltage is due to the insulating effect of pericardial effusion, and the ST elevation reflects inflammation of the pericardium. These findings, in conjunction with clinical signs of heart failure, support a diagnosis of pericarditis.
References:
- https://www.researchgate.net/figure/Figure-5-Ultrasonogram-in-a-cow-affected-with-fibrinous-pericarditis-On-the-outside_fig8_233814025
- Braun, U., et al. “Traumatic pericarditis in cattle: clinical, radiographic and ultrasonographic findings.” The Veterinary Journal 179.3 (2009): 482-492.PubMed+3ResearchGate+3zora.uzh.ch+3
- Ibrahim, H., & Gomaa, N. A. “Traumatic Pericarditis in Cattle: Risk Factors, Clinical Features and Ultrasonographic Findings.” ResearchGate (2016).ResearchGate+1ResearchGate+1
- Ahmed, F. A. “Ultrasonogram in a cow affected with fibrinous pericarditis.” ResearchGate (2011).
- Tharwat, M. “Traumatic Pericarditis in Cattle: Sonographic, Echocardiographic and Pathologic Findings.” ResearchGate (2011).ResearchGate
- Vetlexicon Bovis. “Pericarditis.” Vetlexicon (2022).Vetlexicon
- The Pharma Journal. “Diagnostic evaluation of pericarditis in cattle.” The Pharma Journal 11.10S (2022): 157-160.The Pharma Journal
- Merck Veterinary Manual. “Traumatic Reticuloperitonitis in Cattle.” Merck Vet Manual (2022).Merck Veterinary Manual
- BMC Veterinary Research. “Cardiac biomarkers as tools in the prediction and diagnosis of traumatic pericarditis and traumatic reticuloperitonitis in cattle and buffaloes.” BMC Vet Res (2024).BioMed Central+2ResearchGate+2ResearchGate+2